Unlike corporate boards, hospital trustees carry an additional layer of obligation: stewardship of community health. That dual role — legal fiduciary and moral guardian of a nonprofit mission — makes governance failures especially consequential.
This guide covers the three foundational fiduciary duties, how they apply across specific oversight domains, ERISA obligations most boards underestimate, personal liability exposure, and practical steps trustees can take today.
Key Takeaways
- Hospital board members carry three core legal duties: care, loyalty, and obedience — each enforceable, not aspirational.
- Fiduciary responsibility extends to financial oversight, patient safety, cybersecurity governance, and ERISA retirement plan management.
- Trustees who breach these duties can face personal financial liability, removal, and reputational harm — even without personal gain.
- Best defense: document every decision, its rationale, and any conflicts of interest disclosed.
The Three Core Legal Fiduciary Duties of Hospital Board Members
Statutory and common law impose three specific duties on all nonprofit board members. In healthcare — where tax-exempt status, federal reimbursement, and patient safety intersect — these duties carry exceptional weight. AHA Trustee Services identifies all three as foundational to hospital governance.
Duty of Care
The duty of care requires trustees to act with the diligence an "ordinarily prudent person" would exercise under similar circumstances. In practice, this means:
- Attending meetings and actively reviewing financial and quality reports
- Asking informed questions — not rubber-stamping leadership's recommendations
- Understanding the material risks the organization faces
- Maintaining baseline financial literacy to interpret statements, KPIs, and risk indicators
California Corporations Code §5231 codifies this standard for nonprofit directors explicitly, requiring that directors act with reasonable inquiry when circumstances warrant. Boards that cannot interpret the documents placed in front of them likely fail this duty.
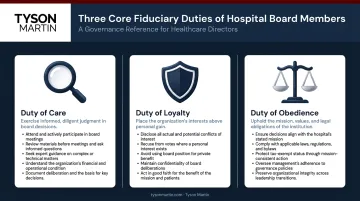
Duty of Loyalty
Trustees must act in the best interests of the hospital and its mission — not in their own personal or professional interests. Practical obligations include:
- Disclosing conflicts of interest promptly and completely
- Recusing from decisions where a conflict exists
- Ensuring the hospital's conflict-of-interest policy is consistently applied
IRS Form 990 Part VI requires hospitals to report governing body composition, family and business relationships among officers and directors, and whether a written conflict-of-interest policy is in place. Even the appearance of self-dealing can invite IRS scrutiny or legal challenge. The disclosure requirement exists because intent is rarely visible from the outside.
Duty of Obedience
Trustees must ensure the hospital operates in accordance with its mission, articles of incorporation, bylaws, and all applicable laws. This is the duty most boards underestimate.
"Mission fidelity" for a nonprofit hospital is not abstract. It encompasses:
- Community benefit obligations and charity care commitments
- Tax-exempt purpose under IRS Revenue Ruling 69-545
- Compliance with Section 501(r), which can trigger a $50,000 excise tax per facility for CHNA failures — and in serious cases, revocation of 501(c)(3) status
Boards that delegate this familiarity entirely to management or outside counsel have no independent basis to catch a mission drift or compliance gap before it becomes a regulatory problem.
Key Fiduciary Responsibility Areas for Hospital Boards
Beyond the three legal duties, hospital boards have specific oversight domains where their accountability is both legally required and ethically unavoidable.
Financial Oversight and Sustainability
Financial fiduciary responsibility means more than approving an annual budget. Trustees must:
- Monitor cash flow and liquidity trends against industry benchmarks
- Understand debt obligations and capital planning assumptions
- Review revenue cycle performance and identify early warning signs of distress
- Ensure independent financial audits are conducted regularly
Fitch reported that median operating margins for nonprofit hospitals recovered to 1.1% in fiscal 2024, up from 0.4% in 2023, with days cash on hand stabilizing at approximately 215 days. Progress, yes. But margins that thin leave almost no buffer. A board that reads only the summary line may miss a deteriorating trend until it becomes a crisis.
Audit committee members need enough expertise to challenge management's representations, not just receive them. The AICPA offers a Not-for-Profit Audit Committee Toolkit specifically designed for nonprofit governing boards — a practical starting point for committees evaluating their own capacity.
Quality and Patient Safety Oversight
Hospital boards have a distinct fiduciary obligation that corporate boards do not: direct oversight of clinical quality and patient safety. Under 42 CFR §482.21, the governing body is explicitly responsible for ensuring QAPI programs reflect the complexity of hospital services.
The gap between what boards should do and what they actually do is documented. A Joint Commission survey found:
- 37% of boards did not include quality performance reviews on every meeting agenda
- 58% spent less than 20% of board time on quality issues
- Only 50% ranked quality as a top governance priority
That matters for outcomes, not just compliance. Research published in PubMed found that board practices — including a dedicated quality committee and linking executive evaluations to safety indicators — were directly associated with better process-of-care and risk-adjusted mortality performance.
Boards that treat quality reporting as a routine agenda item rather than an active accountability function are the ones most likely to face regulatory scrutiny when outcomes deteriorate.
Cybersecurity and Technology Governance
PHI breaches increased from 216 in 2010 to 566 in 2024, with hacking and IT incidents now accounting for 81% of all healthcare breaches. Those numbers explain why cybersecurity is no longer an IT department concern — it is a board-level fiduciary obligation. The Change Healthcare cyberattack demonstrated the systemic exposure: 94% of hospitals reported financial impact, and nearly 60% reported revenue losses of $1 million per day or more.
OCR holds leadership accountable for governance failures, not just technical ones. The duty of care requires the board to understand cyber risk at an oversight level.
The board's role in cybersecurity is distinct from management's:
| Board Governance | Management Operations |
|---|---|
| Set risk appetite and thresholds | Run the security program |
| Approve funding for risk reduction | Manage day-to-day controls |
| Receive credible, decision-ready reporting | Report progress and escalate |
| Approve exceptions when business accepts risk | Own execution and remediation |
| Oversee incident readiness | Operate the response plan |

That division of responsibilities only works if the board can evaluate whether the reporting it receives is meaningful. A dashboard of metrics that no one on the board can interpret or act on does not fulfill the duty of care — it creates the appearance of oversight without the substance. For boards without internal cybersecurity expertise, an independent board advisor provides the translation layer that makes genuine oversight possible: clear risk appetite language, decision rights that hold under pressure, and reporting structured around what changed and what action is required.
Tyson Martin's advisory work focuses on exactly this gap — helping boards receive cyber reporting they can use, not technical briefings they have to take on faith. His contributions to NACD and the World Economic Forum's Centre for Cybersecurity are grounded in the same governance architecture.
ERISA and Retirement Plan Fiduciary Obligations
Most hospital boards focus governance energy on clinical and financial oversight — and overlook a legally distinct category of risk sitting in the HR department: ERISA.
Hospitals sponsoring 403(b) or 401(k) retirement plans are subject to independent fiduciary duties under 29 U.S.C. §1104, which requires fiduciaries to act solely in participants' interests, with care and prudence, including diversifying investments to minimize large-loss risk.
The litigation exposure is real and growing. According to Goodwin's 2025 ERISA Litigation Update, there were 38 ERISA class-action settlements challenging plan fees and investments in 2024, totaling approximately $174 million.
Health systems are direct targets. Rush University Medical Center settled an ERISA lawsuit involving its defined-contribution plan for $2.95 million in 2022.
The primary liability driver is hidden fees embedded in fund expenses. Plaintiff attorneys have become sophisticated at identifying excessive costs that plan sponsors failed to monitor.
That monitoring gap is where board-level accountability begins. Trustees should be able to answer each of these questions affirmatively — and in writing:
Governance checklist:
- Does a formal committee own retirement plan oversight with documented authority?
- When was the last comprehensive fee and service analysis conducted?
- Is there a written investment policy statement?
- Are investment selections reviewed and documented on a recurring schedule?
- Can the organization produce records showing the process — not just the outcomes?

The DOL's prudence standard focuses on process and documentation, not investment results alone. A plan that loses money isn't automatically a liability. A plan that was never systematically reviewed almost certainly is.
Personal Liability: Consequences of Breaching Fiduciary Duty
Fiduciary duty is legally enforceable. Trustees who breach their obligations may be held personally liable to restore losses to the organization or the retirement plan — without any requirement that they personally profited.
Courts can also remove fiduciaries from their roles and impose equitable remedies. The foundational hospital case, Stern v. Lucy Webb Hayes (1974), established that hospital trustees are held to a high standard of care and may face personal liability for negligent fiduciary management.
Co-fiduciary liability adds another layer of exposure. Under 29 U.S.C. §1105, a trustee who knows another board member is breaching a duty and fails to act may bear liability alongside them. Accountability runs peer-to-peer across the board, not only downward to management — and the law treats silence as complicity.
The protections available:
The business judgment rule shields trustees who can demonstrate they:
- Acted in good faith
- Made decisions on an informed basis
- Honestly believed the decision served the organization's best interests
Documentation is the primary evidence courts rely on when evaluating this standard. Board minutes, records of questions asked, disclosed conflicts, and the basis for decisions are the concrete record courts examine when assessing whether the standard was met.
D&O liability insurance and separate fiduciary liability coverage provide additional protection layers, but neither eliminates the underlying duty or the need for documented process.
How Hospital Board Members Can Fulfill Their Fiduciary Duties
Active engagement — not passive attendance — is the baseline. Trustees must participate substantively in meetings, ask questions that require real answers, and insist that reporting is contextual and actionable rather than voluminous and opaque. Three areas define what that engagement looks like in practice: ongoing education, disciplined documentation, and the right board composition.
Ongoing Education
Healthcare governance evolves rapidly. Reimbursement models, cybersecurity threats, HIPAA requirements, and value-based care structures all shift in ways that affect what informed oversight looks like. The AHA's 2026 National Governance Report found that 91% of hospital boards now track clinical quality as a key performance indicator — but tracking a metric and understanding what drives it are different things.
NACD publishes a 2026 Director's Handbook on Cyber-Risk Oversight providing principle-based guidance for directors. AHA Trustee Services publishes hospital-specific cybersecurity resources for trustees. These are not optional background reading — they define what informed oversight looks like to regulators and courts.
Documentation as Defense
Document everything that matters:
- Meeting attendance and participation
- Decisions made and the substantive basis for them
- Conflicts of interest disclosed and how they were handled
- For retirement plans: investment policy statements and periodic review records
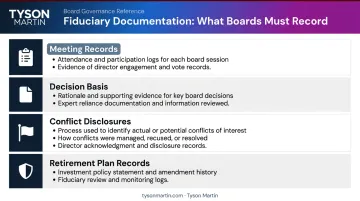
For cybersecurity governance specifically, boards should be able to produce records of risk discussions, tabletop participation, investment approvals, and documented thresholds. When OCR or CMS calls, documentation is what separates a defensible governance record from an indefensible one.
Board Composition and External Advisors
Relevant expertise on the board directly determines fiduciary capacity. Boards should include members with substantive backgrounds in:
- Finance and audit
- Law and regulatory compliance
- Clinical quality
- Technology and cybersecurity
Where internal expertise is unavailable — and for cybersecurity, it often is — engaging an independent external advisor fills the gap without requiring the board to become technical. An advisor like Tyson Martin provides boards with a plain-English view of risk posture, clear decision rights, and independence from internal security teams and vendors — the combination that makes oversight credible rather than ceremonial.
Frequently Asked Questions
What are the fiduciary duties of a board of directors?
Board directors carry three core legal fiduciary duties: care, loyalty, and obedience. These require acting prudently, prioritizing the organization's interests over personal gain, and ensuring compliance with applicable laws and governing documents. For nonprofit hospitals, all three carry additional weight given tax-exempt status and public health obligations.
What are the responsibilities of a hospital governing board?
The governing board sets strategic direction, oversees financial sustainability, ensures quality and patient safety, hires and evaluates the CEO, and maintains regulatory compliance. The key distinction is governance versus management — boards hold accountability for outcomes, not day-to-day operations.
Can a hospital board member be held personally liable for breach of fiduciary duty?
Yes. Trustees can face personal financial liability to restore losses to the organization or retirement plan, even without personal gain. The business judgment rule offers protection when trustees act in good faith and on an informed basis — so documenting the decision-making process is essential.
How does ERISA apply to hospital board members?
Hospitals sponsoring 403(b) or 401(k) plans are subject to ERISA fiduciary requirements, including the duty to monitor investment options, ensure fees are reasonable, and document ongoing oversight. Personal liability is possible for failures in process — not just investment outcomes.
What is the board's fiduciary role in hospital cybersecurity?
As cyber threats to healthcare escalate, boards have a duty of care obligation to ensure adequate oversight — including setting risk appetite, requiring clear reporting, and confirming governance structures are funded and accountable. The board's job is to ensure management owns the security program and answers for it, not to run it directly.