Introduction
Hospital boards carry legal accountability for outcomes they often don't see clearly until the damage is done. By the time the board learns about it, the exposure has already compounded:
- A patient safety incident surfaces first in a malpractice filing
- A ransomware attack hits the news before it reaches the boardroom
- A regulatory penalty arrives months after the compliance failure was flagged and shelved
The tension isn't a lack of effort. Most hospital boards receive risk reports. The problem is that receiving a report and exercising genuine oversight are two very different things.
According to The Joint Commission's 2023 board resource, 72% of hospital board members are not confident in their ability to guide safety and quality oversight — and 58% spend less than 20% of meeting time on quality-related issues. The issue isn't access to information. It's whether the board has the structure to act on it.
What follows is a practical breakdown of what genuine board-level risk oversight looks like in hospitals: the fiduciary duties at stake, what belongs in a credible risk report, and the practices that distinguish resilient boards from reactive ones.
Key Takeaways
- Hospital boards have legal fiduciary duties — Care, Loyalty, and Obedience — that require active oversight, not passive receipt of updates
- Effective board risk reports cover clinical safety, regulatory compliance, financial exposure, operational resilience, and technology/cyber risk
- Best practices include selective reporting, trend dashboards, pre-defined escalation triggers, and corrective action tracking with named owners
- Technology and cyber risk is the most consequential and least well-governed domain at most hospital boards
What Hospital Risk Management Means at the Board Level
Hospital risk management, at the board level, is the process of identifying, evaluating, and reducing threats to patients, staff, financial stability, and regulatory standing. The board's role in that process is strategic oversight — not operational execution.
That distinction matters. The board doesn't run the compliance program or manage incidents day-to-day. It sets the conditions under which management does that work well.
The Five Risk Domains That Belong in Governance Discussions
The AHA's 2024 ERM Boardroom Brief identifies risk domains hospital boards should have visibility into as a strategic discipline integrated with performance. All five need to appear in governance discussions — not just patient safety:
- Clinical and patient safety risk — sentinel events, near-misses, quality metrics
- Regulatory and compliance risk — HIPAA, CMS conditions, Joint Commission standards
- Financial risk — reimbursement exposure, fraud, reserve adequacy
- Reputational risk — public incidents, workforce trust, community relationships
- Technology and cyber risk — ransomware, data breaches, vendor dependencies, system downtime

Many hospital boards still treat cyber and technology risk as an IT problem. It isn't. When a ransomware attack shuts down electronic health records, care delivery stops. That's a patient safety event with financial and regulatory consequences — and a board-level issue, full stop.
The Board's Fiduciary Duties in Healthcare Risk Oversight
The Three Duties and What They Require
AHA's board fiduciary guidance identifies three core legal duties for healthcare board directors:
- Duty of Care — Act with the diligence of a reasonably prudent person. Review data critically, ask substantive questions, and follow up when something is unclear — not just sign off on the agenda
- Duty of Loyalty — Put the organization's interests first. Patient safety and institutional integrity take precedence over personal, political, or external interests
- Duty of Obedience — Ensure the organization operates within applicable laws and its stated mission. Regulatory compliance, HIPAA, CMS conditions, and Joint Commission standards aren't optional
Together, these duties mean a board that receives a risk report, notes it in the minutes, and moves on isn't exercising governance — it's creating a paper trail. Active oversight looks different.
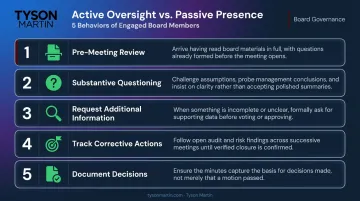
Active Oversight vs. Passive Presence
Active oversight has specific behaviors attached to it. Board members are expected to:
- Review key reports critically before meetings, not during them
- Ask substantive questions — "What changed since last quarter? What decision do you need?"
- Request additional information when something doesn't add up
- Track corrective actions to completion, with named owners and deadlines
- Document what was decided, not just what was presented
The OIG's compliance guidance for healthcare boards identifies asking the right questions of management as a core board obligation. Defensible oversight shows evidence of engagement: questions documented, actions tracked, decisions recorded.
Setting Risk Appetite and Governance Structure
Active oversight requires a clear risk appetite to anchor it. The board is responsible for defining how much risk the organization will accept across different domains — a hospital might hold high tolerance for clinical innovation and very low tolerance for data security failures or financial fraud. That appetite needs to be stated explicitly, with thresholds defined, not implied.
The governance structure supporting this should include:
- A designated risk or audit committee with a clear charter and reporting cadence
- Defined roles for who generates risk data, who reviews it, who escalates it
- Documented thresholds distinguishing management-level responses from board-level notifications
- A process for reviewing and updating appetite as strategic priorities change
Without documented escalation thresholds, boards routinely learn about significant incidents through news coverage rather than internal channels.
What Belongs in a Hospital Board Risk Report
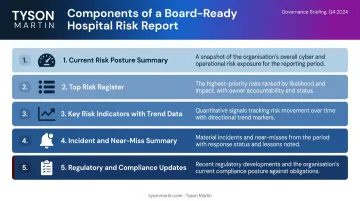
The Core Components
A well-structured hospital board risk report covers five areas:
- Current risk posture summary — plain-language statement of where the organization stands and what changed since last time
- Top risk register — five to ten active risks with status, trend direction, and a named mitigation owner
- Key risk indicators with trend data — not snapshot figures, but movement over time
- Incident and near-miss summary — with root cause status and any open corrective actions
- Regulatory and compliance updates — Joint Commission, HIPAA, CMS changes affecting current exposure
The Joint Commission also recommends annual written reports covering system or process failures, sentinel events, proactive safety actions, improvement project counts, and staffing adequacy analyses.
Why Trend Data Matters More Than Point-in-Time Numbers
A board that sees medication error rates declining for three consecutive quarters makes fundamentally different strategic decisions than one reviewing a single quarter's figure in isolation. One data point can mislead. A trend line shows whether a risk is resolving or building.
Cyber and compliance metrics follow the same principle. Static snapshots — "we had X incidents this quarter" — tell the board almost nothing. Whether that number is improving, stable, or worsening is what governance actually requires.
Calibrating Detail for Board Consumption
Most board members are not clinical or technical specialists. A 2023 study of 15 top-ranked U.S. hospitals found only 14.6% of board members were health professionals. Reports need to translate technical risk data into strategic implications — not operational metrics.
The distinction: a board doesn't need infection rate calculations. It needs to know whether infection-related risk is in or out of risk appetite, what management is doing about it, and whether a decision or policy direction is required.
What the Report Should Ask of the Board
A risk report is not informational only. Each report should identify specific decisions, approvals, or policy directions the board needs to provide. Boards that receive reports without clear asks tend to engage less meaningfully — and produce less defensible documentation of oversight.
Every board-ready dashboard should close with a clear ask — not just a status update. If the report doesn't identify what the board needs to decide, it isn't finished.
Best Practices for Hospital Board Risk Reporting
Report Selectively
Boards are most effective when reports focus on material risks requiring strategic attention. Not every operational metric belongs at the board level. Compliance officers and risk managers should filter what rises to the board versus what stays at the management tier.
If a metric can't answer "in appetite or out of appetite," it belongs in management reporting.
Establish a Consistent Cadence With Defined Escalation Triggers
Quarterly formal reporting keeps the board informed. But quarterly isn't enough on its own. Boards need pre-documented thresholds that trigger off-cycle briefings. Examples include:
- A sentinel event or unexpected patient death
- A ransomware attack or confirmed data breach
- A significant regulatory finding or enforcement action
- A vendor incident affecting critical care systems
- Any event where the financial or operational impact exceeds management's delegated decision authority
Without these thresholds documented before an incident occurs, escalation becomes a judgment call under pressure. Critical information gets filtered before it ever reaches the board.
Link Risk to Strategy
Every material risk presented to the board should connect to the strategic objective it threatens or the regulatory requirement it implicates. "Medication reconciliation errors are increasing" is operational information. "This trend creates Joint Commission re-accreditation exposure and threatens the planned expansion of the surgical program" is governance information.
Require and Track Corrective Action Plans
Effective board oversight means following up, not just receiving. The board should confirm that action plans from prior reports have:
- Named ownership assigned to a specific role, not a committee
- Defined timelines with measurable milestones
- Clear criteria for what "closed" means
- Status updates at each subsequent meeting until the risk is resolved or formally downgraded
A 90-day structured plan format works well here: stabilization in the first 30 days, executive alignment and decision-making in days 31–60, and locked-in execution with ownership in days 61–90.
Build Board Literacy on Key Risk Domains
The AHA's 2022 National Health Care Governance Survey found that 61% of hospital and health system boards had no continuing education requirement for board members. The Joint Commission's 2023 data found only 29% of boards receive continuous education on quality and safety.
Boards that don't understand the risk landscape — including evolving cyber threats and regulatory changes — cannot provide meaningful oversight. Director education doesn't require technical expertise. It requires enough fluency to:
- Ask the right questions when risk is presented
- Interpret trend data rather than accept summaries at face value
- Recognize when management's answers are incomplete or conflict with prior reporting
Technology and Cyber Risk: The Board Oversight Gap in Hospitals
The Scale of the Problem
Hospitals are high-value ransomware targets. Their technology infrastructure intersects directly with patient safety. Yet most board risk reports treat cyber as an IT department issue.
The numbers are stark. According to HHS OCR's 2024 breach report, 663 large breach notifications affected 242.9 million individuals — with hacking and IT incidents representing 81% of large breach reports. IBM's 2024 data puts the average healthcare data breach cost at $9.77 million, the highest of any industry for the fourteenth consecutive year.
A peer-reviewed study of ransomware attacks on U.S. healthcare delivery organizations found annual attacks more than doubled from 2016 to 2021, with care disruptions including electronic system downtime, canceled procedures, and ambulance diversion. These are patient safety events. They're also board-level events.

What Board-Level Cyber Oversight Should Cover
Plain-language reporting on cyber risk for a hospital board should include:
- Current threat posture — what the organization faces and how exposure has changed
- Incident and near-miss history — what happened, what the response was, what's still open
- HIPAA and regulatory compliance status — including any open enforcement activity or unresolved findings
- Third-party and vendor risk — which critical vendors introduce the most exposure
- Active remediation status — what's being fixed, by whom, and on what timeline
The AHA's board cybersecurity guidance notes that board members should understand who is responsible for cybersecurity and incident response, when the board will be notified of intrusions or breaches, which committee oversees cyber risk, and whether management has evaluated the NIST Cybersecurity Framework.
Even well-structured checklists don't close the oversight gap on their own — which is exactly where most hospital boards find themselves stuck.
Bridging the Technical-Governance Gap
The most common failure in hospital board cyber reporting is that the information is built to inform rather than to support decisions. Boards see what's green, what's in progress, and what's planned. They still can't answer the questions that matter: What could stop operations? What risk has management accepted? What do you need from us?
Tyson Martin works with boards and executive teams to translate technical risk posture into governance-level decisions, establish inspectable reporting frameworks, and build escalation thresholds that hold under real incident pressure. Engagements produce:
- A plain-English risk posture summary with changes since the last briefing
- A one-page dashboard with trend indicators (not trivia)
- Decision rights mapped to escalation tiers
- A structured corrective action plan with named owners and measurable outcomes
Common Failures in Hospital Board Risk Governance
Vanity Metrics and Activity Reporting
Boards that receive reports showing "policies reviewed" or "training completion rates" are measuring activity, not risk reduction. Completing 99% of annual HIPAA training and still experiencing a breach isn't a paradox — it's what happens when activity metrics substitute for outcome metrics.
Instead, replace activity counts with metrics that show direction:
- Are critical vulnerabilities on the highest-risk systems being remediated faster?
- Is detection coverage on key attack paths improving?
- Is the time between incident detection and containment shrinking?
If a metric doesn't change a decision, it's not a key risk indicator. It's noise.
No Defined Escalation Path
When an incident occurs and the board asks "why didn't we hear about this sooner," the answer is almost always that escalation thresholds were never formally defined. Without documented decision rights — what management handles versus what requires board notification — important information gets filtered out before it reaches governance.
A well-structured escalation model distinguishes between events management can contain within operational thresholds versus events that cross materiality lines:
- Financial impact above a defined dollar threshold
- Exposure of regulated patient or operational data
- Disruption to critical care systems
- Any situation where decision authority exceeds management's delegated limits
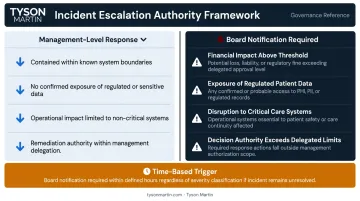
Time-based triggers matter too. A prolonged incident with uncertain scope should automatically escalate even if initial impact appears contained.
Treating Risk Reporting as a Compliance Checkbox
The most common failure is a board that receives risk updates, notes them in minutes, and moves on without meaningful discussion, follow-up, or accountability. This behavior creates documentation of receipt, not documentation of oversight.
Risk oversight that holds up in a regulatory review or legal proceeding demonstrates engagement: questions asked and documented, actions tracked to completion, decisions recorded with named owners. The Mid Staffordshire NHS Trust public inquiry — a landmark hospital governance failure — showed exactly what happens when information is filtered through subcommittees and boards become distanced from operational reality. The board received reports, reviewed them, and recorded no meaningful response — and patients paid for that gap.
Frequently Asked Questions
What is the board's role in hospital risk management?
The board's role is strategic oversight: setting risk appetite, approving the governance framework, reviewing risk reports, and holding management accountable for execution. It does not manage incidents or run the compliance program day-to-day — that's management's job. The board's obligation is to ensure management does it well.
How often should hospital boards receive risk management reports?
Most hospitals provide formal risk reports quarterly. That cadence should be supplemented by pre-documented escalation triggers requiring off-cycle briefings for sentinel events, ransomware or breach incidents, significant regulatory findings, or any event that crosses the organization's materiality thresholds.
What should a hospital board risk report include?
A board risk report should include a current risk posture summary, a top risk register with trend data and named owners, key risk indicators showing movement over time, an incident and near-miss summary with root cause status, and regulatory updates — all framed at a strategic level with clear asks for board decision or direction.
What is the difference between a hospital risk committee and full board risk oversight?
A risk or audit committee performs deeper, more frequent review of risk data and brings prioritized findings to the full board. The full board retains ultimate fiduciary responsibility but delegates detailed analysis to the committee. The committee digs in; the board makes final calls on material risks and governance decisions.
How should hospital boards oversee technology and cybersecurity risk?
Boards should receive regular plain-language briefings on cyber threat posture, HIPAA compliance status, incident history, and vendor exposure — with technical findings translated into strategic implications. A board advisor or fractional CISO who operates at the governance level, not the technical one, closes the gap between what management knows and what the board can act on.
What are the most common failures in hospital board risk reporting?
Three failures show up repeatedly: reporting activity metrics instead of risk outcomes, missing pre-defined escalation thresholds that specify what requires board notification, and treating risk updates as informational rather than requiring documented decisions with named accountability for open items.